Free NACC Practice Questions on Delirium (Ontario PSW Exam Prep)
If you are studying for the NACC Personal Support Worker (PSW) exam in Ontario, delirium is one of the highest-yield clinical topics you can review — many long-term care and home-care clients are older adults, and the PSW who provides their daily care is almost always the first to notice that a client is "not themselves" today. This free practice set gives you real NACC-style questions on telling delirium from dementia, the sudden change from baseline, UTIs and other reversible causes, hypoactive versus hyperactive delirium, why you never restrain, and the changes to report, each with a clear answer. Work through them, then keep going with the full question bank at pswleap.com/learn.
What is delirium on the NACC PSW exam?
For the exam, delirium is a sudden change in a client's mental state — new confusion, poor attention, and an alertness that comes and goes — that the PSW must recognize and report quickly, because it is often caused by something treatable. The "right answer" in a delirium question almost always combines noticing the change from the client's normal baseline, keeping the client safe without restraint, and reporting promptly to the nurse. Delirium lives inside the cognitive and mental-health part of PSW practice, but it carries its own urgency that the exam likes to test.
The reason it matters: the PSW knows what "normal" looks like for each client, so they catch the moment a client slips — and that early catch makes the difference.
Delirium, dementia, and the "three Ds"
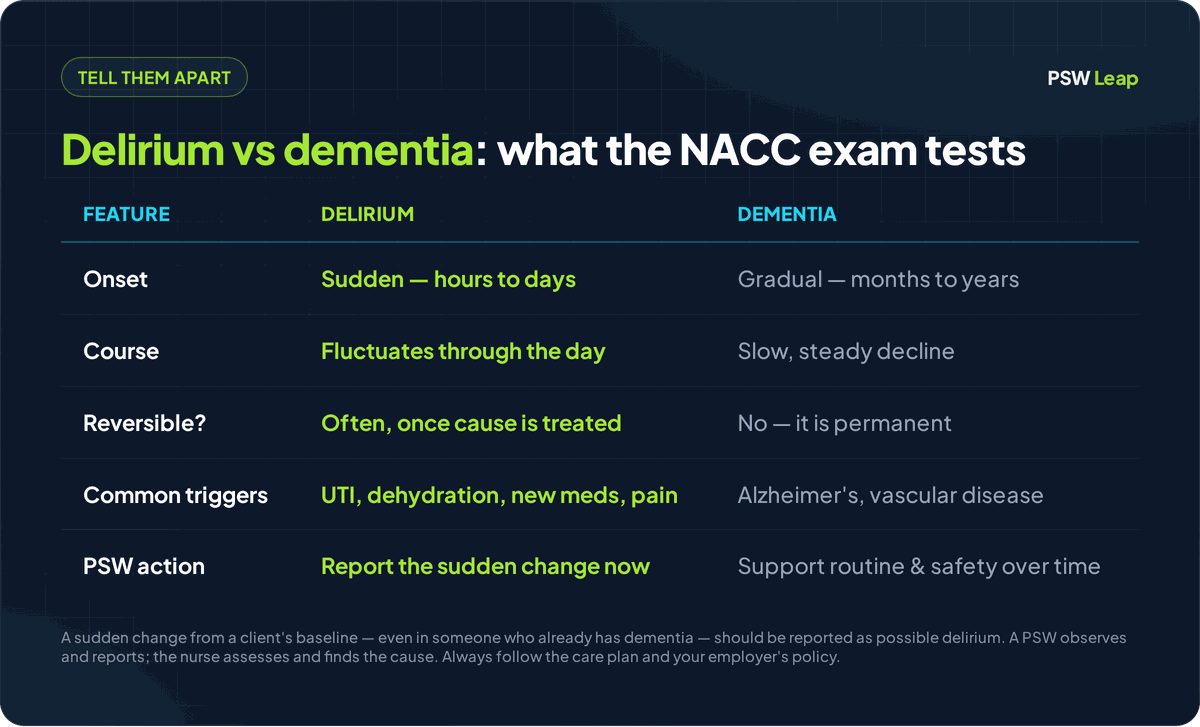
The biggest clue that separates delirium from dementia is how fast it started. Delirium comes on suddenly — over hours or a few days — and fluctuates, often worse in the late afternoon or at night, and it is usually reversible once the cause is treated. Dementia comes on gradually — over months and years — as a slow, permanent decline. Depression, the third of the "three Ds," affects mood and energy and can also look like confusion in an older adult. The exam tests whether you can tell sudden, treatable confusion apart from a long-standing condition.
The trap the exam loves: a client with known dementia who suddenly becomes much more confused or agitated than their usual self. The wrong instinct is to shrug and say "that's just the dementia." The right move is to treat the sudden worsening as a possible delirium layered on top of the dementia — and report it, because a treatable cause is often hiding underneath.
The PSW's role in Ontario: notice the change, keep them safe, report
A PSW observes and reports a sudden mental-status change; the nurse assesses, finds the cause, and decides on treatment. In Ontario, a PSW works from the client's individual care plan and the employer's policies, within the controlled-acts limits of the Regulated Health Professions Act, 1991. Watching for changes, keeping a client safe and calm, supporting hydration and comfort, and reporting clearly are all routine PSW tasks. Diagnosing the cause, ordering or giving medication, and applying restraints are not — those belong to the nurse and the care team.
Two scope points the exam rewards. First, a sudden change in mental state is never a "wait and see" — the PSW reports it promptly to the registered nurse or registered practical nurse. Second, restraint is a last resort, not a first response: under Ontario's least-restraint approach, the team tries everything else first, and any restraint must be ordered.
Quick terms to know: Baseline = what is normal for this client — their usual alertness and behaviour. Delirium = sudden, fluctuating confusion that is often reversible. Hyperactive delirium = the agitated, restless, sometimes-hallucinating kind. Hypoactive delirium = the quiet, withdrawn, sleepy kind (easily missed). Reversible = able to get better once the cause is treated. Least restraint = trying every other option before any restraint is even considered.
Free NACC-style practice questions: delirium
Each question below mirrors the scenario-based, multiple-choice style of the NACC PSW exam. Try to answer before you read the explanation.
Q1. A client who is normally alert becomes confused, drowsy, and unsure where she is over the course of an afternoon. What does this most likely suggest, and what should the PSW do?
Answer: This is a sudden change suggesting delirium — report it to the nurse promptly. Confusion that comes on over hours, in a usually-alert client, is the classic picture of delirium. Because it is often caused by something treatable, the PSW keeps the client safe and reports the change right away.
Q2. What is the main difference between delirium and dementia?
Answer: Delirium comes on suddenly and is often reversible; dementia comes on gradually and is a permanent decline. Onset speed is the biggest clue: hours-to-days and fluctuating points to delirium; months-to-years of slow decline points to dementia. A client can have both at once.
Q3. A client with known dementia is far more confused and agitated today than his usual self. What should the PSW assume?
Answer: Don't assume "it's just the dementia" — report the sudden change. A quick worsening from a client's baseline can be delirium on top of dementia, often from a treatable cause like an infection. The PSW reports it so the nurse can look for what changed.
Q4. Which common, treatable problem often shows up as sudden confusion in an older client?
Answer: A urinary tract infection (UTI). In older adults a UTI can cause sudden confusion, sometimes before any pain or fever. Other common reversible causes include dehydration, constipation, a new medication, and pain. The PSW reports the confusion; the nurse looks for the cause.
Q5. A usually-chatty client has become very quiet, withdrawn, and sleepy — not herself at all. Why does this matter?
Answer: This can be hypoactive (quiet) delirium, which is easily missed — report it. Because the client isn't disruptive, quiet delirium often gets mistaken for tiredness. But sudden quiet confusion is still delirium and still needs the nurse's attention.
Q6. A confused client keeps trying to climb out of bed and is agitated. The care plan does not order a restraint. What should the PSW do?
Answer: Do not restrain — stay with the client, keep them safe, and call the nurse. Restraints can make delirium worse and are a last resort that must be ordered. The PSW reduces noise, removes hazards, reorients gently, and keeps the client company while reporting.
Q7. What everyday measures can a PSW use to help prevent or ease delirium?
Answer: Glasses and hearing aids in, fluids within the care plan, calm light by day and dark and quiet by night, familiar objects, gentle reorientation, and staying mobile. These simple supports lower the risk of confusion, and the exam expects the PSW to know them.
Q8. A PSW notices a sudden mental-status change in a client. What is the single most important action?
Answer: Report it to the nurse promptly. Delirium is not "wait and see." Early reporting lets the team find and treat the cause before the client gets worse, which is the whole reason the PSW's daily watchfulness matters.
Q9. How should a PSW document a client who has suddenly become confused?
Answer: Record the facts — the client's usual baseline, what changed, when it started, exactly what you observed, and the client's own words in quotes. The PSW does not guess at the cause; that is the nurse's job. Clear, objective, time-stamped notes help the team act quickly.
Q10. A client becomes newly confused on the evening shift, a day after a fall. Is this expected, and what should the PSW do?
Answer: New confusion after a fall, surgery, an infection, or a medication change is a red flag for delirium — report it. It may be common, but it is never "just normal." The PSW keeps the client safe and tells the nurse rather than writing it off as tiredness.
Common delirium mistakes to avoid on the NACC exam
- Dismissing a sudden change as "just the dementia" instead of reporting it as possible delirium on top of the dementia.
- Missing the quiet kind — assuming a withdrawn, sleepy client is only tired, when hypoactive delirium looks exactly like that.
- Restraining an agitated, confused client instead of staying with them and calling the nurse — restraint is a last resort and must be ordered.
- Treating a sudden mental-status change as "wait and see" rather than reporting it promptly.
- Guessing at or "treating" the cause — the PSW observes and reports; diagnosing and treating belong to the nurse and the care team.
The delirium facts the NACC exam expects you to know
Use these one-line facts as a final review:
- Sudden change = report now — new confusion over hours or days is not "wait and see."
- Delirium is sudden and often reversible; dementia is gradual and permanent — onset speed is the clue, and a new worsening in a client with dementia can be delirium on top.
- UTIs, dehydration, constipation, new medications, and pain are common, treatable causes — the PSW reports, the nurse finds the cause.
- Quiet (hypoactive) delirium is the easily-missed kind — withdrawn and sleepy still counts.
- Never restrain a confused client as a first response — keep them safe, reorient gently, call the nurse.
- Support the basics — glasses and hearing aids in, fluids, day-and-night light cues, familiar objects, mobility.
- A PSW observes and reports; the nurse assesses, finds the cause, and treats.
Remember: PSW practice in Ontario always follows the client's individual care plan and your employer's policies, within the controlled-acts limits of the Regulated Health Professions Act, 1991. Recognizing and reporting delirium is within a PSW's role; diagnosing it, treating it, and ordering restraints are not. This article is exam-prep study material, not medical advice.
Practice more free NACC questions
You just answered 10 delirium questions, and the NACC exam spans every module. The fastest way to find your weak spots is to keep practising with instant feedback.
👉 Start practising free at pswleap.com/learn — a large bank of NACC-style questions, full timed mock exams, and a Duolingo-style study path built specifically for Ontario PSW students. No subscription, and you can start with sample questions before you pay.
Closely related topics worth reviewing next: Free NACC Practice Questions on Dementia Care (the long-standing condition delirium is so often confused with) and Free NACC Practice Questions on Restraints & Least Restraint (why "keep them safe" never means "tie them down").
PSW Leap is an independent NACC PSW exam-prep platform for Ontario candidates. We are not affiliated with NACC. Always follow your training, your client's care plan, and your employer's policies on the job.
Published by PSW Leap
Independent NACC PSW exam prep
PSW Leap articles are written and maintained by the platform's founder, Shashank Jha, and checked against publicly available PSW curriculum standards. Found an error? Email hello@pswleap.com and we'll fix it.
Read our content methodologyPSW Leap
Practice smarter for the NACC exam. 2,400+ questions. Detailed rationales. $29.99 CAD one-time — everything included.
Try 10 free questions →No account needed. Ready for the full bank? Create your account.