Free NACC Practice Questions on COPD & Chronic Respiratory Care (Ontario PSW Exam Prep)
If you are studying for the NACC Personal Support Worker (PSW) exam in Ontario, chronic obstructive pulmonary disease (COPD) is one of the conditions you will meet most often — in home care, retirement homes, and long-term care. This free practice set gives you real NACC-style questions on the tripod position, pursed-lip breathing, home oxygen safety, the flare-up signs you must report, and the PSW's observe-and-report scope — each with a clear answer. Then keep going at pswleap.com/learn.
What is COPD and respiratory care on the NACC PSW exam?
For the exam, caring for a client with COPD means helping them breathe more easily and conserve energy within the care plan — using positioning and pursed-lip breathing, following the prescribed oxygen, watching for a flare-up, and reporting changes — without changing the oxygen or treating the client yourself. COPD is a long-term lung disease (mainly chronic bronchitis and emphysema, most often from years of smoking) that makes it hard to push air out, leaves the client short of breath, and slowly worsens.
Positioning and breathing techniques that ease shortness of breath
When a client with COPD is breathless, sit them upright and lean them slightly forward, and coach pursed-lip breathing — both ease the work of breathing without any equipment. The tripod (orthopneic) position — sitting up and leaning forward with the arms resting on a table, a pillow, or the knees — lets the breathing muscles work better. Never lay a breathless COPD client flat.
Pursed-lip breathing is the technique the NACC exam expects you to know: the client breathes in gently through the nose, then breathes out slowly through pursed lips, like blowing out a candle. Breathing out slowly keeps the airways open longer, helps empty the trapped air, and calms the panic that comes with breathlessness. A PSW coaches and reminds the client to use it; the technique is first taught by the nurse or respiratory therapist.
Home oxygen: keeping it safe, and the PSW's role
Follow the prescribed oxygen flow exactly, never change it, and keep everything that burns well away — because oxygen feeds fire. The flow rate, such as 2 litres per minute, is a physician or respiratory-therapist order. In COPD, turning the oxygen up can be dangerous, so the PSW never adjusts it: if the client is more breathless even on oxygen, keep the prescribed flow and report to the nurse.
Oxygen makes any fire burn faster and hotter, so keep the client and equipment away from smoking, open flames, candles, gas stoves, and heaters — usually at least three metres. Store cylinders upright and secured, keep the tubing untangled and unkinked so the flow is not blocked, and check the skin behind the ears and under the nose where the cannula presses. Use a water-based lip balm, not a petroleum one. In Ontario, home oxygen is often funded through the Assistive Devices Program (ADP) and supplied by a vendor, with day-to-day support arranged through Ontario Health atHome — report any equipment problem to the nurse or the oxygen vendor.
Energy conservation and the breathlessness–anxiety cycle
Pace every task, sit for care, and exhale on effort so the client spends less breath on daily activities. A client with COPD tires quickly, so break tasks into small steps with rest breaks, use a shower chair for washing, gather supplies before you start, and keep everyday items within easy reach. Teach the client to breathe out during the hard part of a movement — for example, exhaling while standing up.
Breathlessness and anxiety feed each other: feeling short of breath causes fear, fear speeds up the breathing, and faster breathing makes the breathlessness worse. When this happens, stay calm, reassure the client, and coach slow pursed-lip breathing to break the cycle. Your own unhurried manner is part of the treatment.
Spotting a flare-up (exacerbation): what to watch for and report
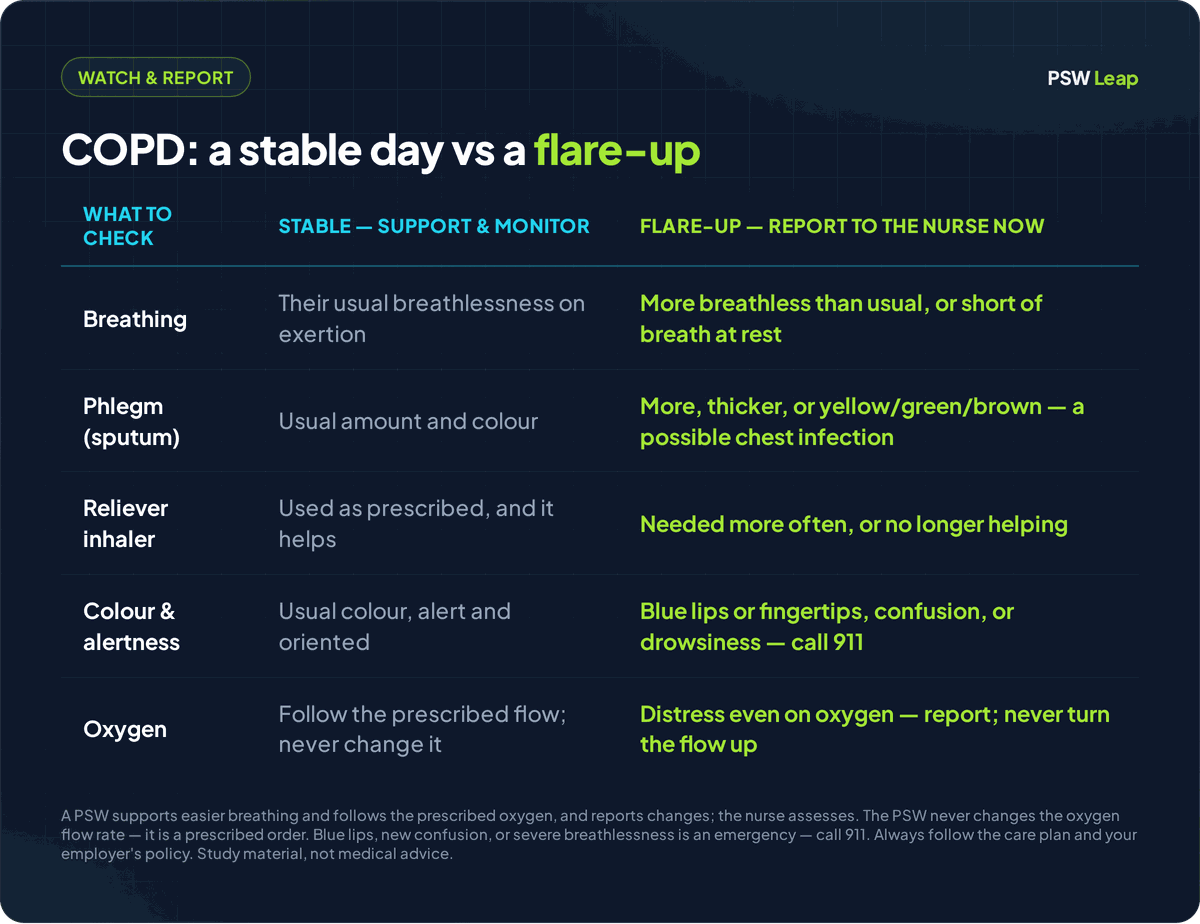
Know the flare-up signs and report them early, because a PSW usually spots the first change. Report when the client is more short of breath than usual or breathless at rest; when the phlegm (sputum) changes — more of it, thicker, or turning yellow, green, or brown, which often means a chest infection; when a rescue (reliever) inhaler is needed more often or stops helping; or when there is new fever, wheeze, or chest tightness.
Some signs are emergencies. Blue lips or fingertips (cyanosis), new confusion or drowsiness, or severe breathlessness that will not settle mean you call 911 and get help immediately. Because chest infections are the most common trigger of a flare-up, hand hygiene and keeping unwell visitors away matter; cold air, smoke, dust, and strong smells can also set one off. The PSW reports early and keeps the client calm; the nurse assesses.
Quick terms to know: COPD = chronic obstructive pulmonary disease, a long-term lung disease that makes breathing out hard. Exacerbation = a flare-up, when symptoms suddenly get worse. Tripod / orthopneic position = sitting up and leaning forward on the arms to ease breathing. Pursed-lip breathing = breathing out slowly through pursed lips. Sputum = phlegm coughed up from the lungs. Cyanosis = a bluish colour of the lips or fingertips from low oxygen. Cannula = the small tubing with prongs that delivers oxygen at the nose.
Free NACC-style practice questions: COPD and respiratory care
Each question mirrors the scenario-based, multiple-choice style of the NACC PSW exam. Try to answer before you read the explanation.
Q1. A client with COPD suddenly becomes very short of breath while sitting in bed. What should the PSW do?
Answer: Help the client sit fully upright and lean slightly forward with their arms resting on a table or their knees (the tripod position), and coach slow pursed-lip breathing. Never lay them flat.
Q2. A client on 2 L/min home oxygen feels more breathless and asks the PSW to "turn the oxygen up." What should the PSW do?
Answer: Do not change the oxygen — keep it at the prescribed 2 L/min and report the increased breathlessness to the nurse. Turning oxygen up in COPD can be dangerous; the flow is a prescribed order.
Q3. A client with COPD is panicking because they cannot catch their breath. What should the PSW do first?
Answer: Stay calm, reassure the client, and coach slow pursed-lip breathing to break the breathlessness–anxiety cycle before it worsens.
Q4. A PSW notices a client's phlegm has changed from clear to thick and green, and there is more of it. What should the PSW do?
Answer: Report the change in sputum to the nurse — more, thicker, or coloured phlegm can be an early sign of a chest infection and a COPD flare-up.
Q5. A client who uses home oxygen wants to light a cigarette. What should the PSW do?
Answer: Do not allow smoking near the oxygen — oxygen feeds fire. Keep all flames and heat sources well away and report the smoking to the care team.
Q6. A client with COPD becomes exhausted every time they shower. How can the PSW best conserve the client's energy?
Answer: Use a shower chair, gather supplies first, work in slow steps with rest breaks, and have the client exhale during the effort. Sitting and pacing lower the demand on their breathing.
Q7. A client with COPD is drowsy and confused, and their lips look bluish. What should the PSW do?
Answer: Treat it as an emergency — call 911 and get help immediately. Blue lips (cyanosis) and new confusion are signs of dangerously low oxygen.
Q8. A client says their reliever inhaler "isn't working" and asks the PSW to change the dose. What should the PSW do?
Answer: Never change an inhaler dose — assist only as the care plan allows, and report to the nurse that the inhaler is not helping.
Q9. Where should the PSW check the skin on a client who wears a nasal oxygen cannula?
Answer: Check behind the ears and under the nose, where the tubing and prongs press, and report any redness or skin breakdown.
Q10. A client with COPD has to travel to an appointment on a cold, windy day. What should the PSW do to protect their breathing?
Answer: Help the client cover the nose and mouth with a scarf so they breathe warmed air — cold air is a common trigger that tightens the airways in COPD.
Common COPD-care mistakes to avoid on the NACC exam
- Turning the oxygen up when a client is more breathless instead of keeping the prescribed flow and reporting.
- Lying a breathless client flat instead of sitting them upright and forward and coaching pursed-lip breathing.
- Ignoring a change in the phlegm's colour or amount instead of reporting a possible chest infection early.
- Allowing smoking, candles, or heaters near oxygen instead of keeping all flames and heat well away.
The COPD facts the NACC exam expects you to know
Use these one-line facts as a final review:
- The two no-equipment fixes — sit upright and lean forward (tripod), and coach pursed-lip breathing — ease breathing in any setting.
- Follow the prescribed oxygen flow exactly and never change it, and keep smoking, flames, and heat well away because oxygen feeds fire.
- Report a flare-up early — more breathlessness, or more, thicker, or coloured phlegm — and call 911 for blue lips, new confusion, or severe distress.
Remember: PSW practice in Ontario follows the client's care plan and your employer's policies, within the controlled-acts limits of the Regulated Health Professions Act, 1991. Positioning, coaching pursed-lip breathing, energy conservation, following the prescribed oxygen, and observing and reporting are within a PSW's role; changing the oxygen flow, assessing the lungs, diagnosing a flare-up, and giving or adjusting inhalers or other medication are not. Assist with medication only as the care plan directs. This article is exam-prep study material, not medical advice.
Practice more free NACC questions
You just answered 10 COPD and respiratory care questions, but the NACC PSW exam spans every module — keep practising to find your weak spots.
👉 Start practising free at pswleap.com/learn — a large bank of NACC-style questions, full timed mock exams, and a Duolingo-style study path built for Ontario PSW students. No subscription needed to start.
Closely related topics worth reviewing next: Free NACC Practice Questions on Oxygen Therapy and Free NACC Practice Questions on Heart Failure Care — the oxygen skills and the overlapping breathlessness that often sit alongside COPD.
PSW Leap is an independent NACC PSW exam-prep platform for Ontario candidates. We are not affiliated with NACC. Always follow your training, your client's care plan, and your employer's policies on the job.
Written by Shashank Jha
Founder, PSW Leap
Shashank Jha is the founder of PSW Leap. He built this platform after going through the NACC exam prep process himself, to help fellow students study smarter with practice questions mapped to every NACC module.
Learn more about PSW LeapPSW Leap
Practice smarter for the NACC exam. 2,400+ questions. Detailed rationales. $29.99 one-time.
Try it now →