PSW Medication Assistance — What You Can and Cannot Do
Medication assistance is one of the most important — and most misunderstood — areas of PSW practice. Module 10 of the NACC curriculum covers this topic in detail, and the certification exam includes scenario questions that test whether you understand the boundary between assisting with medication and administering medication. Getting this wrong on the exam costs you marks. Getting it wrong in practice can cost a client their health.
This guide explains exactly what you can and cannot do with medications as a PSW in Ontario, the 6 Rights of medication that apply to every medication interaction, delegation and assignment rules, documentation requirements, and the common medication errors that show up on the NACC exam.
The Fundamental Rule: Assist, Do Not Administer
The single most important concept to understand about PSW medication scope is the distinction between assisting and administering.
Assisting with medication means helping a client take medication that has already been prescribed and prepared by a regulated health professional. You are acting as an extension of the prescriber's order, under the direction of a nurse or other regulated professional.
Administering medication means independently deciding what medication to give, preparing it, calculating doses, or performing controlled acts like injections. This is outside the PSW scope of practice.
Think of it this way: you are the last set of hands in a chain that starts with the physician's order and passes through the pharmacist and nurse. Your role is to ensure the right client receives the right medication at the right time in the right way — and to observe and report.
The 6 Rights of Medication
The 6 Rights are your safety checklist for every single medication interaction. Before assisting any client with any medication, you must verify all six:
-
Right Client — Confirm the identity of the person receiving the medication. Use at least two identifiers (name, date of birth, room number, photo). Never assume — always verify, even with clients you know well.
-
Right Medication — Verify that the medication matches what is listed on the medication administration record (MAR) or the pharmacy label. If the name, appearance, or packaging looks different from what you expected, stop and check with the nurse.
-
Right Dose — Confirm that the amount matches the order. If a blister pack contains a different number of pills than expected, or if the dose looks different from usual, report it before proceeding.
-
Right Time — Give the medication at the time specified in the care plan or MAR. "Right time" generally means within 30 minutes before or after the scheduled time. Some medications must be given at precise times or in relation to meals (before, with, or after food).
-
Right Route — Confirm how the medication should be taken. Common routes include oral (by mouth), sublingual (under the tongue), topical (applied to the skin), ophthalmic (eye drops), otic (ear drops), and inhaled. Never change the route without direction from the nurse.
-
Right Documentation — Record that the medication was given, including the time, the client's response, and any refusals or concerns. Documentation must be completed immediately after the medication is taken — not at the end of your shift.
Some programs and workplaces add a 7th Right — Right Reason — which means understanding why the medication has been prescribed. You do not need to know pharmacology in depth, but knowing that a medication is for blood pressure, pain, or anxiety helps you observe for expected effects and potential problems.
You are assisting Mrs. Garcia with her morning medications. The blister pack is labelled with her name and contains four pills. The MAR indicates she should receive three pills at 0800. What should you do?
What PSWs CAN Do
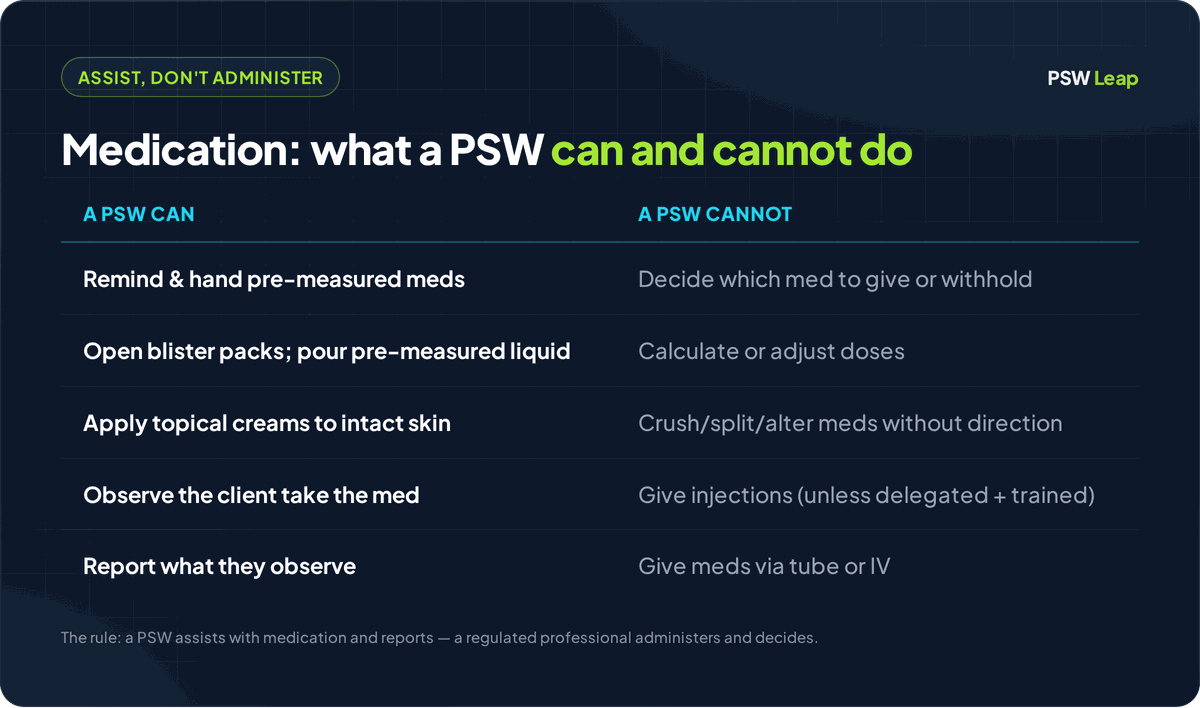
Within your scope, you may perform the following medication-related tasks when directed by a regulated health professional and consistent with employer policies:
- Remind the client that it is time to take their medication
- Open child-proof containers or blister packs that the client cannot open themselves
- Hand pre-packaged, pre-measured medication to the client
- Pour a pre-measured liquid medication into a cup for the client
- Observe the client take the medication (ensure they swallow it, do not pocket it in their cheek, and do not choke)
- Apply topical medications (creams, ointments, patches) to intact skin as directed in the care plan
- Administer eye drops, ear drops, or nasal sprays after receiving specific training and competency assessment, and only when delegated
- Assist with metered-dose inhalers (puffers) according to the care plan
- Document the medication assistance on the MAR or other designated form
- Observe and report any side effects, adverse reactions, or changes in the client's condition after taking medication
- Store medications properly (locked cabinet, correct temperature, away from light if required)
What PSWs CANNOT Do
The following are outside the PSW scope of practice and must never be performed unless a specific delegation has been made by a regulated health professional (and even then, only with proper training and documentation):
- Decide which medication to give or withhold
- Calculate or adjust medication doses
- Crush, split, or alter medications without specific direction from the nurse or pharmacist
- Give injections (insulin, heparin, or any other injectable medication) — unless specifically delegated with training
- Administer medications through tubes (nasogastric, gastrostomy, or jejunostomy tubes)
- Administer intravenous (IV) medications or adjust IV flow rates
- Administer controlled substances (narcotics, opioids) without direct nursing supervision
- Administer PRN (as-needed) medications without direction from the nurse for each specific occurrence — the PSW cannot independently assess whether a PRN medication is needed
- Accept verbal or telephone orders from a physician or nurse practitioner
- Repackage medications from one container to another
Delegation vs. Assignment
Understanding the difference between delegation and assignment is essential for the NACC exam and for practice.
Assignment is when a regulated health professional directs you to perform a task that is already within your scope of practice. No special authority is being transferred — you are simply being told to do something you are trained and authorized to do. Example: the nurse assigns you to assist Mr. Lee with his morning blister pack medications.
Delegation is when a regulated health professional authorizes you to perform a task that is normally outside your scope of practice. The regulated professional retains accountability for the outcome. Delegation requires:
- A specific order from the delegating professional
- Training in the specific skill being delegated
- Competency assessment — the delegating professional must verify that you can perform the task safely
- Ongoing supervision — the delegating professional must be available for questions and must periodically reassess your competency
- Documentation of the delegation, training, and competency assessment
- Employer policy that permits delegation for that specific task
For example, a home care nurse may delegate insulin injection to a PSW for a specific client. The nurse would provide training, observe the PSW performing the injection, document the delegation, and remain available by phone. The PSW would only perform this task for this specific client under this specific delegation — it does not extend to other clients or other medications.
Key exam point: If a task has been delegated to you, you have the right to refuse if you do not feel competent or if the situation has changed (for example, the client's condition has worsened). You should communicate your concerns to the nurse.
A home care nurse has delegated insulin administration to a PSW for Mrs. Wong. The PSW arrives at Mrs. Wong's home and finds her blood sugar reading is significantly lower than usual. What should the PSW do?
High-Alert Medications
High-alert medications are drugs that carry an increased risk of causing significant harm if they are used in error. While PSWs do not independently manage these medications, you should be able to recognize them and understand why extra caution is needed.
Common high-alert medications you may encounter:
- Insulin — errors in dosing can cause dangerously low blood sugar (hypoglycaemia), leading to confusion, seizures, or death
- Anticoagulants (blood thinners) such as warfarin — overdose can cause life-threatening bleeding; underdose can lead to blood clots
- Opioids (morphine, hydromorphone, fentanyl) — overdose can cause respiratory depression and death
- Cardiac medications (digoxin, antiarrhythmics) — dosing errors can cause dangerous heart rhythms
- Hypoglycaemic agents (oral diabetes medications) — can cause dangerously low blood sugar
When assisting with high-alert medications, apply the 6 Rights with extra vigilance and report any unusual observations immediately.
Medication Storage
Proper medication storage is within the PSW's responsibility and is tested on the NACC exam.
- Locked storage — All medications in long-term care and many community settings must be stored in a locked cabinet or drawer. Narcotics require a double-locked system.
- Temperature — Most medications are stored at room temperature (15-25 degrees Celsius). Some medications (such as insulin and certain antibiotics) require refrigeration. Check the label.
- Light protection — Some medications must be stored away from direct light (nitroglycerin, for example).
- Expiry dates — Check expiry dates regularly. Never assist a client with expired medication — report it to the nurse.
- Separation — Keep internal medications (taken by mouth) separate from external medications (applied to the skin or used in the eyes/ears).
- Client-specific — Never use one client's medication for another client, even if it is the same medication and dose.
Common Medication Errors
Understanding common medication errors helps you prevent them in practice and answer exam questions correctly.
| Error Type | Example | Prevention |
|---|---|---|
| Wrong client | Giving Mrs. Smith's medication to Mrs. Smythe in the next bed | Always use two identifiers before assisting |
| Wrong time | Giving the evening dose at lunch because you forgot earlier | Follow the MAR schedule; set reminders if needed |
| Wrong dose | Giving two pills when the order is for one | Check the MAR against the blister pack every time |
| Wrong route | Having a client swallow a sublingual medication | Confirm route on the MAR; know what "sublingual" means |
| Omission | Forgetting to give a medication entirely | Use the MAR as a checklist; sign off after each medication |
| Documentation error | Signing that medication was given before the client actually takes it | Document immediately after — never before or hours later |
If a Medication Error Occurs
If you realize a medication error has been made:
- Check the client — Assess whether the client is showing any adverse effects
- Report immediately — Tell the nurse right away, even if the client seems fine
- Document — Record exactly what happened, when, and what actions were taken
- Do not hide the error — Concealing a medication error puts the client at risk and is a serious professional and ethical violation
- Participate in review — The team will review the incident to prevent future errors, not to punish
Ready to practice?
Medication scope questions are among the trickiest on the NACC exam. Practise with scenario-based questions that test the boundaries of what PSWs can and cannot do.
Start Practising FreePRN Medications — A Special Note
PRN (pro re nata, or "as needed") medications are prescribed to be given only when certain symptoms are present — for example, acetaminophen for pain, lorazepam for anxiety, or an antacid for heartburn.
The key rule for PSWs: you cannot independently decide when a PRN medication is needed. Even if the client tells you they are in pain and asks for their pain medication, you must contact the nurse. The nurse will assess the client, decide whether the PRN medication is appropriate, and direct you to assist with it.
In home care settings where the nurse is not physically present, the process is the same — you call the nurse, describe what you are observing, and wait for direction before assisting with the PRN medication.
Insulin — Understanding Your Boundaries
Insulin comes up frequently on the NACC exam because it sits right at the boundary of PSW scope. Here is what you need to know:
- Insulin is a high-alert medication — dosing errors can be immediately life-threatening
- Insulin administration involves an injection, which is a controlled act under the Regulated Health Professions Act (RHPA) in Ontario
- In most long-term care settings, insulin is administered by the nurse, not the PSW
- In home care settings, insulin administration may be delegated to a PSW by a regulated health professional, with specific training, competency assessment, and ongoing supervision
- If insulin is delegated to you, the delegation is client-specific — it does not authorize you to give insulin to other clients
- You must be trained in blood glucose monitoring, recognizing signs of hypoglycaemia and hyperglycaemia, and knowing when to hold the insulin and call the nurse
Key Takeaways
- PSWs assist with medication; they do not independently administer medication.
- The 6 Rights (Right client, Right medication, Right dose, Right time, Right route, Right documentation) are your safety checklist for every medication interaction.
- Delegation allows a regulated health professional to authorize you to perform tasks outside your usual scope, with training, assessment, supervision, and documentation.
- High-alert medications (insulin, anticoagulants, opioids) require extra vigilance.
- PRN medications require nursing assessment and direction before each use.
- Medication errors must be reported immediately — never concealed.
- When in doubt, stop and ask the nurse. It is always better to pause and clarify than to proceed and cause harm.
For a broader understanding of your scope of practice as a PSW, see our guide on PSW scope of practice in Ontario. For exam-specific strategies, check out how to pass the NACC PSW exam.
Frequently Asked Questions
Written by Shashank Jha
Founder, PSW Leap
Shashank Jha is the founder of PSW Leap. He built this platform after going through the NACC exam prep process himself, to help fellow students study smarter with practice questions mapped to every NACC module.
Learn more about PSW LeapPSW Leap
Practice smarter for the NACC exam. 2,400+ questions. Detailed rationales. $29.99 one-time.
Try it now →